SIMPLE:
A simple pneumothorax occurs when air gets trapped between the potential space of the visceral and parietal pleural. This causes compression of the lung and can cause pain and shortness of breath. Signs include decreased breath sounds on the affected side, tachycardia, tachypnoea, resonance on percussion and occasionally subcutaneous emphysema.

Diagnosis is with chest X-ray.
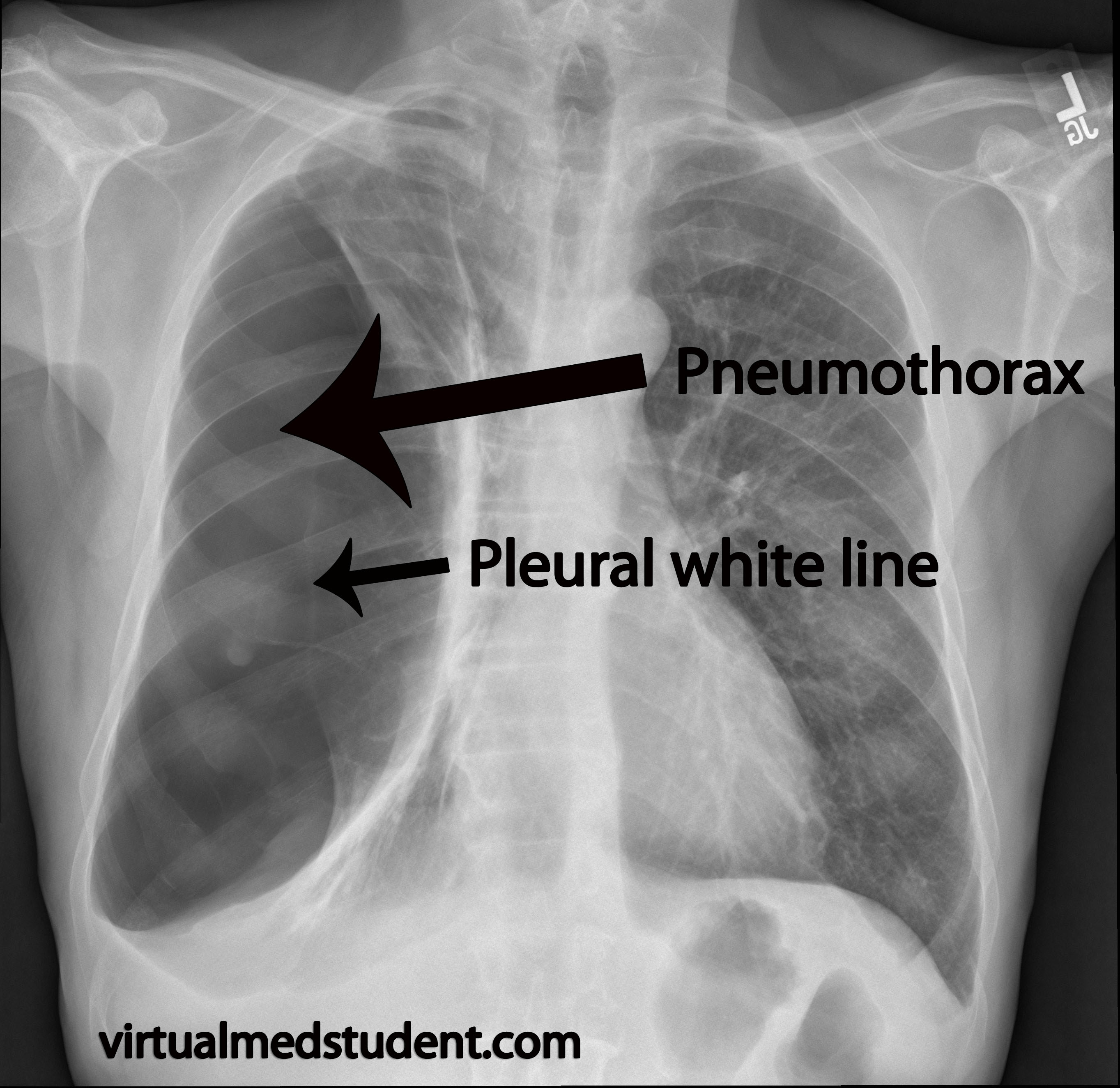 |
| XR of Pneumothorax |
Treatment:
- Administering 100% Oxygen
- Insertion of a tube thoracostomy
- This can be a small calibre tube as there is only air in the pleural cavity. Consider a large bore tube if pleural effusion, haemothorax, or chylothorax also present.
- If persistent, surgical methods may be required to control the pneumothorax
- VATS and pleurodesis - either powder or mechanical
- Pleurectomy
TENSION PNEUMOTHORAX:
This is when a one way valve effect causes air to rapidly build up in the pleural cavity without the ability to be released, causing pain and severe SOB. The compression effect causes a variety of physiological changes, the most severe being cardiogenic shock due to compression of the heart from the air. This results in decreased cardiac output as the heart is unable to be filled and can rapidly lead to collapse and death. Signs of a tension pneumothorax include the above as well as a deviated trachea to the contralateral side of the lesion, hyper-resonance on the affected side, raised JVP and haemodynamic instability.
Diagnosis is clinical.
Treatment:
- Immediate insertion of a needle thoracostomy
- Large bore IV cannula is placed in the mid-clavicular line, 2nd intercostal space
- Correct placement is confirmed with hissing sound of air escaping
- Follow up with definitive tube thoracostomy

OPEN PNEUMOTHORAX:
An open pneumothorax is when there is a free communication with the external environment resulting in the body's inability to generate negative intra-thoracic pressure leading to respiratory fatigue and eventually failure.
Diagnosis is clinical
Treatment:
- Fashioning of a 3 way flap to cover the opening
- This allows air to be pushed out during expiration but stops air from entering during inspiration and allows adequate negative intra-thoracic pressure for inspiration
- Follow up with definitive tube thoracostomy
No comments:
Post a Comment